English
English  中文简体
中文简体 
HOME / NEWS / Industry News / Medical Swabs for PCR Testing: Types, Selection Factors and DNA Collection
Content
What Is a Swab Test and What Is Swab Testing?
A swab test is a diagnostic sampling procedure in which a sterile absorbent-tipped applicator is inserted into or pressed against a body site — most commonly the nasopharynx, oropharynx, wound, or urogenital tract — to collect biological material: cells, mucus, exudate, or microbial organisms. The collected specimen is then submitted for laboratory analysis, which may include culture and sensitivity testing, rapid antigen detection, polymerase chain reaction (PCR) amplification, or genomic sequencing.
Swab testing became familiar to the general public during the COVID-19 pandemic, when nasopharyngeal and anterior nasal swabs were used at population scale for SARS-CoV-2 PCR and rapid antigen testing. In clinical and laboratory practice, however, swab testing encompasses a much broader range of applications: throat swabs for Group A Streptococcus, wound swabs for bacterial culture and antibiotic sensitivity, cervical swabs for HPV and STI screening, buccal swabs for DNA collection in forensic and genetic testing, and environmental swabs in pharmaceutical and food manufacturing quality control.
The swab itself — its tip material, shaft material, and overall geometry — directly affects the diagnostic validity of the test. A swab that collects insufficient sample, retains too much analyte in the tip matrix, or introduces inhibitors into the downstream assay can produce false-negative results or degraded PCR amplification regardless of the laboratory technique applied. Swab selection is therefore a controlled variable in the testing workflow, not an interchangeable commodity.

Medical Swab Tip Types: Foam, Cotton, and Flocked Compared
The three dominant tip constructions in clinical and laboratory swabs — foam, cotton fiber, and flocked nylon — differ fundamentally in how they collect, retain, and release specimen material. Understanding these differences is essential for matching swab type to application.
Cotton-Tipped Swabs
Traditional cotton swabs use a wound or twisted cotton fiber matrix bonded to a wooden or plastic shaft. Cotton is highly absorbent — it draws fluid into the fiber matrix by capillary action — but its absorbency is also its primary limitation for molecular diagnostics. Cotton fiber retains a significant fraction of the collected specimen within the matrix, making elution into transport media or PCR buffer incomplete. Studies comparing swab types for viral recovery have consistently shown cotton swabs release 30–50% less nucleic acid into elution fluid than flocked swabs under matched conditions. Cotton also contains trace PCR inhibitors (tannins and other organic compounds from natural fiber processing) that can reduce amplification efficiency in low-concentration samples. Cotton swabs remain appropriate for culture-based microbiology, wound sampling, and applications where nucleic acid recovery is not the primary concern, but they are increasingly replaced by synthetic alternatives in molecular diagnostic workflows.
Foam-Tipped Swabs
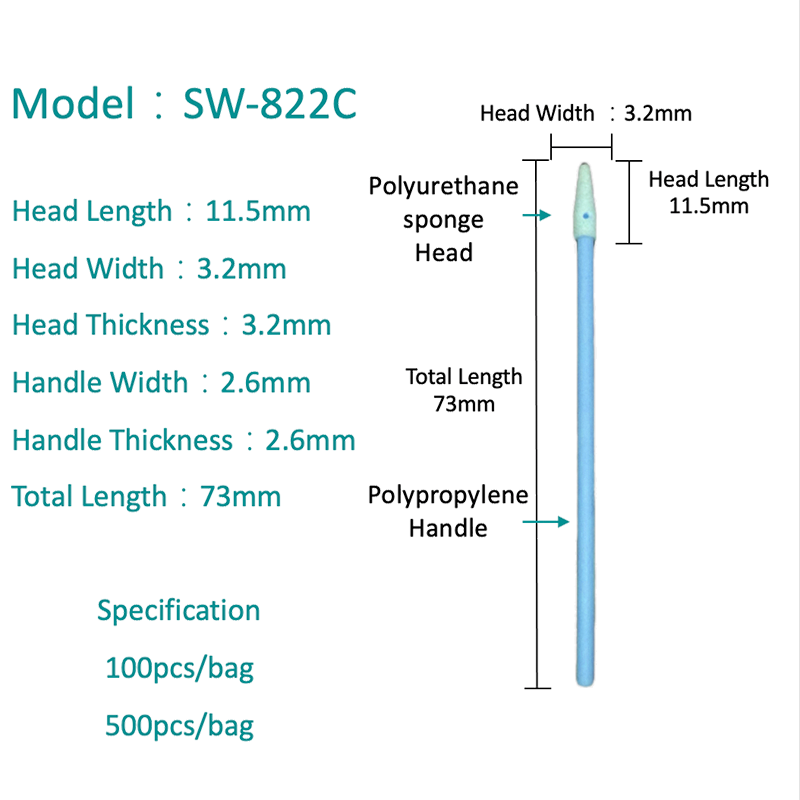
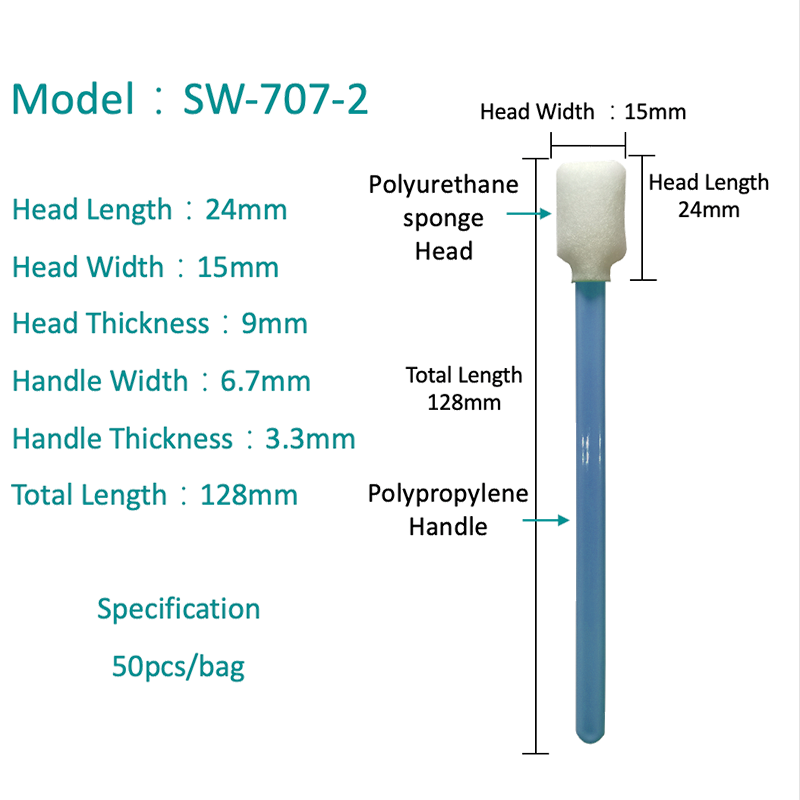
Foam swabs use an open-cell polyurethane or polyester foam tip that absorbs fluid through the interconnected pore structure. Foam tips have a larger contact surface area than wound cotton at equivalent tip dimensions and provide consistent absorption across the tip face, making them effective for surface wipes, wound sampling, and applications requiring high liquid volume collection. High-absorption foam swabs are particularly effective for environmental monitoring and wound exudate collection, where the volume of material present is not limiting. For PCR and molecular testing, foam performs better than cotton — it contains no PCR inhibitors and releases specimen material more completely — but still retains more material in the pore matrix than flocked tips. Foam swabs are also used extensively in forensic sampling of hard surfaces and in electronics and precision component cleaning where controlled absorption is needed.
Flocked Swabs
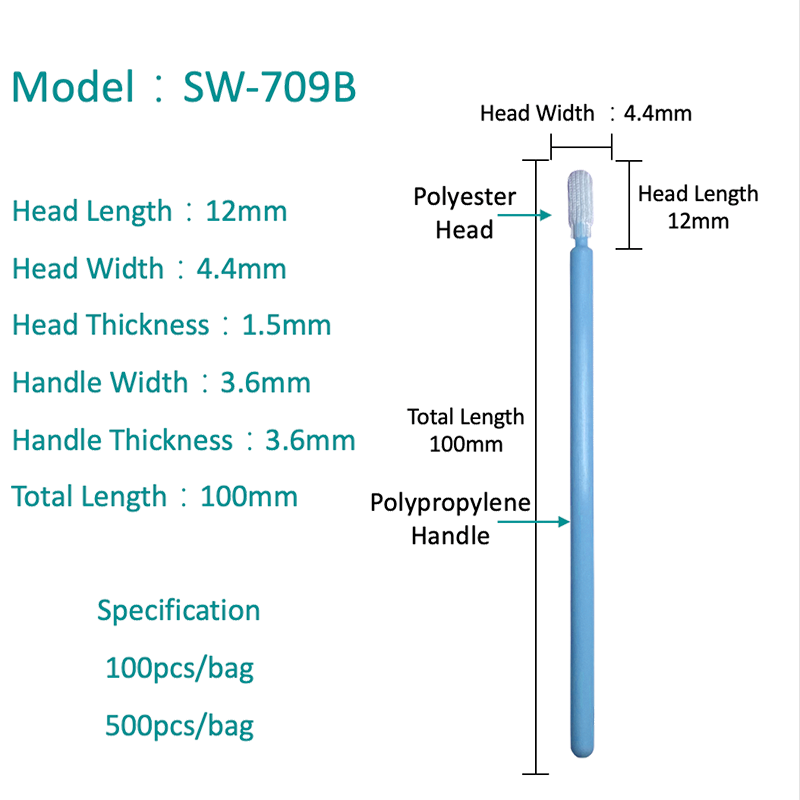
Flocked swabs are the current gold standard for molecular diagnostics and PCR-based testing. The tip is constructed by electrostatically applying perpendicular nylon fibers to an adhesive-coated substrate — creating a velvet-like surface of upright fiber bundles rather than an absorbent matrix. This geometry means specimen material is collected into the spaces between fibers at the tip surface rather than being absorbed into a sponge or fiber matrix. When the swab tip is agitated in elution buffer or transport media, hydraulic release of specimen is near-complete — typically 80–95% elution efficiency compared to 50–70% for foam and under 50% for cotton. For viral, bacterial, and cellular sample collection where maximum nucleic acid recovery determines test sensitivity, flocked swabs consistently outperform the alternatives. They are the recommended swab type for nasopharyngeal collection in COVID-19, influenza, RSV, and other respiratory pathogen PCR testing.
| Property | Cotton | Foam | Flocked Nylon |
|---|---|---|---|
| Collection mechanism | Fiber absorption | Pore absorption | Surface entrapment |
| Elution efficiency | Low (~40–50%) | Moderate (~60–70%) | High (80–95%) |
| PCR inhibitors | Yes (tannins, organics) | None | None |
| Cell collection (genomic DNA) | Moderate | Moderate–High | High |
| Liquid volume capacity | Moderate | High | Low–Moderate |
| Best application | Culture, wound, general | Environmental, wound, forensic | PCR, molecular, genomic DNA |
Most Reliable Medical Swabs for PCR Testing
For PCR-based diagnostic testing, the swab must maximize the number of intact cellular and viral particles delivered to the extraction step, and must introduce no chemical inhibitors that reduce polymerase activity or nucleic acid binding in the extraction protocol. This points consistently to flocked nylon nasopharyngeal or nasal swabs in sterile viral transport media (VTM) or universal transport media (UTM) as the most reliable configuration for respiratory pathogen PCR.
Several specific design factors distinguish high-reliability PCR swabs from general-purpose alternatives:
- Breakpoint shaft: Nasopharyngeal swabs designed for PCR have a defined breakpoint scored into the shaft, allowing the tip to snap cleanly into the transport tube after collection without the collector needing to cut the shaft. This ensures the tip is fully submerged in transport media and eliminates contamination risk from external shaft surfaces.
- Flexible shaft material: Nasopharyngeal swabs require a shaft flexible enough to navigate the nasal passage to the posterior nasopharynx — typically 15 cm depth — without causing patient injury. Nylon-coated wire or medical-grade polypropylene shafts provide the necessary combination of flexibility and column strength to reach target depth.
- Sterility and DNase/RNase-free certification: PCR swabs must be gamma-irradiated or EO-sterilized and certified free of DNase, RNase, and human DNA — any residual nucleic acid contamination from the manufacturing process can produce false positives in highly sensitive assays.
- Compatibility with transport media: The swab tip material must be compatible with the specific VTM or UTM formulation used downstream. Some foam materials can leach compounds that interact with VTM preservatives; flocked nylon is inert to the full range of standard transport media formulations.
- IVD or CE marking: For clinical use, PCR swabs should carry IVD (In Vitro Diagnostic) classification under FDA 21 CFR Part 820 or CE marking under EU IVDR 2017/746 as applicable to the target market. These designations confirm the swab has been validated for diagnostic specimen collection in a regulated manufacturing environment.
For anterior nasal swabs — used in point-of-care rapid antigen testing and some PCR protocols where nasopharyngeal collection is impractical — midturbinate flocked swabs provide a balance of patient comfort and adequate cellular yield. Anterior nasal flocked swabs are shorter (typically 7–9 cm vs 15 cm for NP swabs) with a smaller, more rounded tip profile and a rigid polypropylene shaft. Their sensitivity for SARS-CoV-2 PCR is lower than matched nasopharyngeal collection — multiple studies place nasal swab sensitivity at 85–92% of nasopharyngeal sensitivity — but this difference is acceptable for population screening and self-testing applications where patient compliance with nasopharyngeal collection is a limiting factor.
Cell Collection for Genomic DNA Testing
Buccal (cheek) swabs are the standard non-invasive collection method for genomic DNA in forensic casework, ancestry testing, pharmacogenomics, clinical genetics, and paternity analysis. The target cells are buccal epithelial cells shed from the inner cheek lining — a continuously renewing surface that yields fresh, nucleated cells with intact genomic DNA under gentle mechanical abrasion.
For genomic DNA applications, flocked or foam swabs outperform cotton significantly because both collect and release more cells per swab and introduce no inhibitors that interfere with downstream DNA extraction chemistry. Flocked swabs are preferred for high-sensitivity applications (single-swab extractions for SNP arrays, whole-genome sequencing, or CODIS STR profiling) because they release cellular material more completely into the extraction buffer during the lysis step. Foam swabs are an acceptable alternative and provide higher total cellular mass when cell yield is the primary concern — the larger contact area and pore volume of a foam tip can collect more total cells from a single cheek wipe than a flocked tip of equivalent dimensions.
Key variables that maximize genomic DNA yield from buccal swabs include: collecting at least 30–60 minutes after eating, drinking, or mouth rinsing (food debris and exogenous DNA dilute the buccal cell population); using firm rotational pressure against the cheek mucosa for 10–15 seconds per swab to maximize epithelial cell abrasion; air-drying swabs fully before sealing into collection envelopes if using dry-transport protocols (moisture promotes bacterial overgrowth, which degrades human DNA); and using two swabs per collection event to ensure sufficient DNA mass for both the primary extraction and an archival reserve.
Factors to Consider When Selecting Medical Swabs
No single swab type serves all clinical and laboratory needs. Selection should be driven by the downstream assay requirement, the collection site anatomy, the transport and storage conditions, and the regulatory context of the testing program.
Downstream Assay Compatibility
Match the swab to the assay: culture requires only clean collection without inhibitors — cotton, foam, or flocked all perform adequately. Molecular assays (PCR, LAMP, NGS) require flocked or inhibitor-free foam swabs in compatible transport media. Rapid antigen tests specify their own validated swab types — using an unvalidated swab with a rapid test kit is a common source of false negatives in point-of-care settings and may invalidate the test under regulatory guidance.
Collection Site Geometry
Shaft length, rigidity, and tip size must match the anatomy of the target collection site. Nasopharyngeal collection requires a 15 cm flexible shaft; wound swabs typically use a rigid 15 cm wooden or polypropylene shaft with a larger tip for surface coverage; buccal swabs use a medium rigid shaft with moderate tip size; urogenital swabs use thin shafts with small tips for patient comfort. Using an inappropriately sized or rigid shaft at a sensitive collection site risks patient injury and compromises sample quality through inadequate tip-to-mucosa contact.
Transport and Storage Requirements
Specimens collected for molecular testing are typically transported in liquid VTM or UTM, which maintains viral and cellular viability at refrigerated temperatures (2–8°C) for 24–72 hours. Dry swab transport — where the swab is returned to its peel-pack or placed in a dry tube without media — is validated for certain molecular assays and is logistically simpler for large-scale collection programs. Not all swab types maintain specimen integrity equally under dry transport; validated dry-transport flocked swabs specify both the swab construction and the storage conditions required to maintain diagnostic sensitivity.
Where to Source Hospital-Grade Medical Swabs
Hospital-grade, high-absorption medical swabs for clinical and laboratory use are available through medical supply distributors (Cardinal Health, Medline, Henry Schein), laboratory reagent and consumable suppliers (Fisher Scientific, VWR, Bio-Techne), and direct from specialized manufacturers (Copan Diagnostics — the developer of flocked swab technology — Puritan Medical Products, and BD Diagnostic Systems). For large-volume procurement, direct manufacturer sourcing provides tighter lot control, validation documentation, and regulatory compliance certificates. For point-of-care and smaller laboratory settings, distributor channels provide broader product range and faster availability. When evaluating suppliers, request lot-level Certificates of Analysis confirming sterility testing, DNase/RNase-free validation, and applicable regulatory clearances (IVD, CE-IVDR, ISO 13485 manufacturing certification) before approving a new swab lot for clinical use.